Download the PDF HERE
How UnitedHealthcare Tried to Imprison a Trans Girl
Metadata, Misgendering, and the Corporate Criminalization of Healthcare Speech
I. Introduction: The Girl, the Phrase, and the Punishment
“Deny. Defend. Depose.”
“Nine more CEOs.”
“Bang bang.”
“I kinda mean that.”
These were not social media threats. Not manifesto language.
These words were spoken—in a private phone call—by a transgender woman calling her health insurer in desperation. She was not threatening anyone. She was begging for care.
Her name is Samara Dorn.
She had just undergone major gender-affirming surgery. Her body was in pain. Her hormone levels were crashing. Her medication was being withheld. And the company charged with protecting her life—UnitedHealthcare—was using every bureaucratic tool at its disposal to delay, deny, and discard her post-operative needs.
She called to protest. She called to plead. She called to survive.
And during that call—a call that was recorded, tagged, and algorithmically scanned—she said those words.
She didn’t say “I’m going to hurt someone.”
She didn’t make a plan.
She didn’t name a target.
She said, “One CEO isn’t enough. Two CEOs isn’t enough. Nine more CEOs.”
She said, “Bang bang.”
She said, “I kinda mean that.”
What she meant was what any critical patient advocate would recognize:
That real change will never come from a single MURDER.
That the corporate rot in American healthcare is systemic.
That it may take multiple heads of a corrupt cartel being removed from power—symbolically, institutionally, legally—before trans people are treated as human.
It was a bitter metaphor.
A rhetorical plea.
A cry of pain from someone who had lost control of her own body at the hands of her insurer.
But UnitedHealthcare didn’t treat it that way.
They didn’t call to follow up. They didn’t send a clinician. They didn’t offer resolution.
They launched a law enforcement escalation.
Surveillance by Proxy
Instead of de-escalating, they escalated her.
Instead of accountability, they initiated containment.
Their internal systems—a mix of keyword flags, call metadata, and behavioral surveillance—red-flagged her as a “risk.” Not based on violence, but on language.
Not based on threat, but tone.
What followed was a two-phase attempt to remove her from the narrative entirely:
UnitedHealthcare made contact with the Department of Homeland Security, reportedly through metadata-driven reporting pathways used by insurers and financial institutions under the guise of “suspicious activity monitoring.”
No imminent threat.
No law enforcement inquiry requested.
Just an inference, passed off as a national security concern.
Thirty-five days later, with no further contact from Samara Dorn, no threatening language, and no ongoing communication, the company transmitted her private health information (PHI) to the Grand Junction Police Department, in a disclosure that violated every procedural safeguard under federal law.
No subpoena.
No warrant.
No verified clinical risk.
No emergency.
The only thing they had was a trans woman, angry and articulate, saying what so many patients silently feel:
“This system is killing us. And it won’t change until the people at the top are forced to face what they’ve done.”
This Was Not a Mental Health Call. It Was a Civil Rights Call.
Samara Dorn wasn’t a threat. She was a whistleblower.
She was a pro se litigant, actively building her legal complaint.
She was citing legal phrases—“Deny. Defend. Depose.”—to describe a known corporate defense strategy.
She was referencing a public scandal involving Luigi Mangione, a health executive whose misconduct had recently come to light.
She was pointing out that one CEO falling isn’t enough to dismantle a billion-dollar apparatus of denial, rationing, and surveillance.
And for this—for saying out loud what others whisper—they treated her as disposable.
What UnitedHealthcare did was not a misunderstanding.
It was not an overreaction.
It was a deliberate attempt to criminalize a patient’s voice by laundering her speech through metadata, recasting advocacy as instability, and treating rhetoric as probable cause.
The Stakes Could Not Be Clearer
Samara Dorn is not alone.
Across the country, trans people face escalating digital profiling, service denial, and “benevolent violence”—where the very institutions meant to protect life weaponize procedure to endanger it instead.
This is the beginning of a pattern.
A warning about what happens when corporate surveillance meets political erasure.
A case study in how trans identity, neurodivergence, and emotional honesty are converted into red flags by systems that mistake pain for threat and truth for instability.
This is the story of how UnitedHealthcare tried to imprison a trans girl—not because she broke the law, but because she named who does.
And now, this paper will do what they feared most.
It will name it again.
Clearly. Publicly. Permanently.
II. Metadata as Judge, Jury, and Executioner
Modern insurance call centers deploy sophisticated metadata surveillance to flag “risky” members—even before any clinician hears the voice on the line. In Samara Dorn’s case, UnitedHealthcare’s systems transformed her private pain call into a criminal referral. Here’s how:
A. Call Tagging and Algorithmic Profiling
Automatic Transcription & Keyword Scanning
Every call is transcribed in real time.
A set of proprietary keywords (e.g., “bang bang,” “CEO,” “threat”) is weighted more heavily when combined with other flags (e.g., mental–health status, gender identity).
As soon as Samara spoke “bang bang” and “nine more CEOs,” the system elevated her “sentiment score” into the danger zone—despite no actual threat language.
Sentiment Analysis & Behavioral Scoring
Beyond keywords, voice analytics estimate emotional distress and anger levels.
High distress + flagged keywords → elevated risk profile.
These “risk scores” routinely trigger automated workflows, including escalation to compliance or “national security” channels.
Networked Suspicious-Activity Reporting
UnitedHealthcare participates in Suspicious Activity Reports (SARs) under the Bank Secrecy Act and related frameworks.
Though originally designed for financial crimes, these SAR-like pathways are repurposed for “unusual” healthcare behavior.
Samara’s call was funneled through the insurer’s compliance team and then to DHS—without ever verifying whether any law had actually been broken.
B. HIPAA’s Emergency Disclosure Rule: Misapplied
Under 45 C.F.R. § 164.512(j), a covered entity may disclose PHI only if all of the following are met:
Good-faith belief of imminent threat
Disclosure is necessary to prevent or lessen that threat
Only the minimum necessary information is shared
Documentation of the basis for the belief and disclosure
UnitedHealthcare’s conduct failed every prong:
No Imminence
Threats must be immediate or impending. Samara’s remarks were metaphorical and abstract—and reported 35 days after the call.
No Necessity
No clinical evaluation or psychiatric consult was performed before or after the disclosure.
Instead of de‐escalation, they opted for law enforcement engagement.
No Minimum Necessary
They forwarded Samara’s entire PHI record, including surgical details, psychiatric notes, medication history, and demographic identifiers—far beyond what a true “emergency exception” would allow.
No Documentation
There is no record of a good-faith belief memo or rationale explaining why these phrases constituted an actual threat.
Internal emails later obtained via CORA show the decision was driven by reputational panic, not clinical judgment.
C. The Corporate-to-Carceral Pipeline
UnitedHealthcare’s metadata surveillance and legal bypass created a playbook for corporate carceral outsourcing:
Surveillance → 2. Flagging → 3. Compliance Escalation → 4. External Referral → 5. Law Enforcement Action
Each step offloads corporate liability onto government actors—but the chain-of-custody remains invisible to the patient:
Surveillance
Patient calls recorded and scored.
Flagging
Keywords + sentiment triggers “high risk” label.
Compliance Escalation
Insurer’s legal/compliance team reviews flagged call, opts for DHS referral.
External Referral
DHS passes on further escalation.
UnitedHealthcare takes a second bite at the apple, and then passes information to Grand Junction Police Department
Law Enforcement Action
Local police draft incident report and — in some cases — consider detention.
By weaponizing routine metadata and misapplying HIPAA’s exception, UnitedHealthcare sought to:
Silence a vocal critic.
Discredit a trans patient by framing her as unstable.
Shift accountability from policy failures to criminal law.
The result: A trans survivor’s private plea for medical care became evidence in a police record—without any legitimate legal or clinical basis. This case exposes a dangerous blueprint for how corporate entities can bypass healthcare and civil–rights protections by outsourcing enforcement to government agencies.
III. From Healthcare to Handcuffs: The Anatomy of Retaliatory Disclosure
UnitedHealthcare didn’t just mishandle a call. They strategically weaponized it—transforming private distress into a pretext for law enforcement involvement. This section breaks down the precise chain of actions that led from a patient’s plea to a retaliatory police report.
A. The Call That Triggered the Machine
Samara Dorn’s call was not spontaneous—it was provoked by UnitedHealthcare’s own conduct:
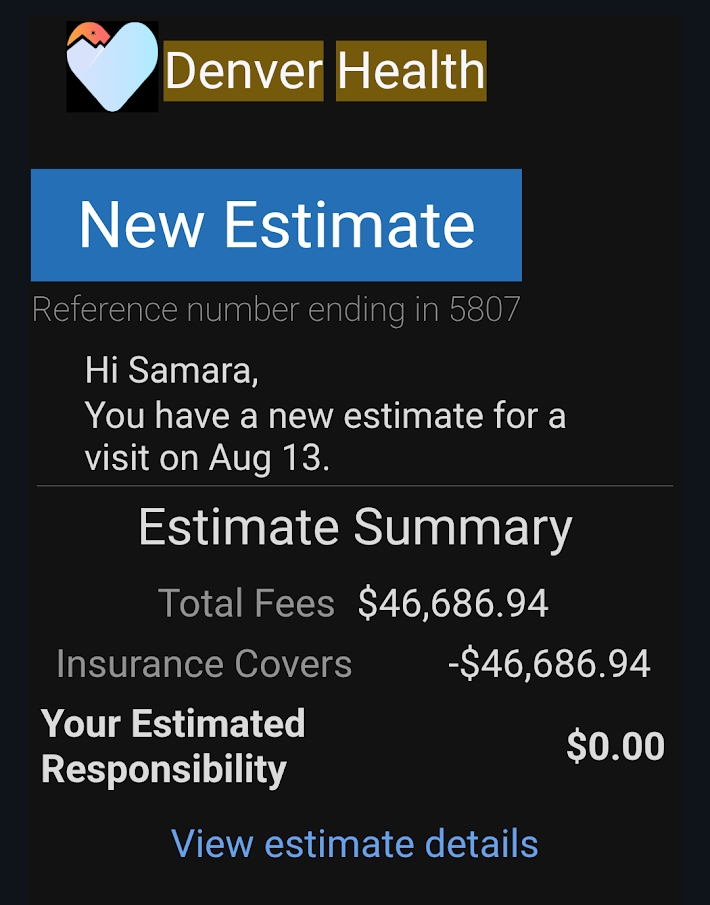
She had undergone major gender-affirming surgery on August 13, 2024.
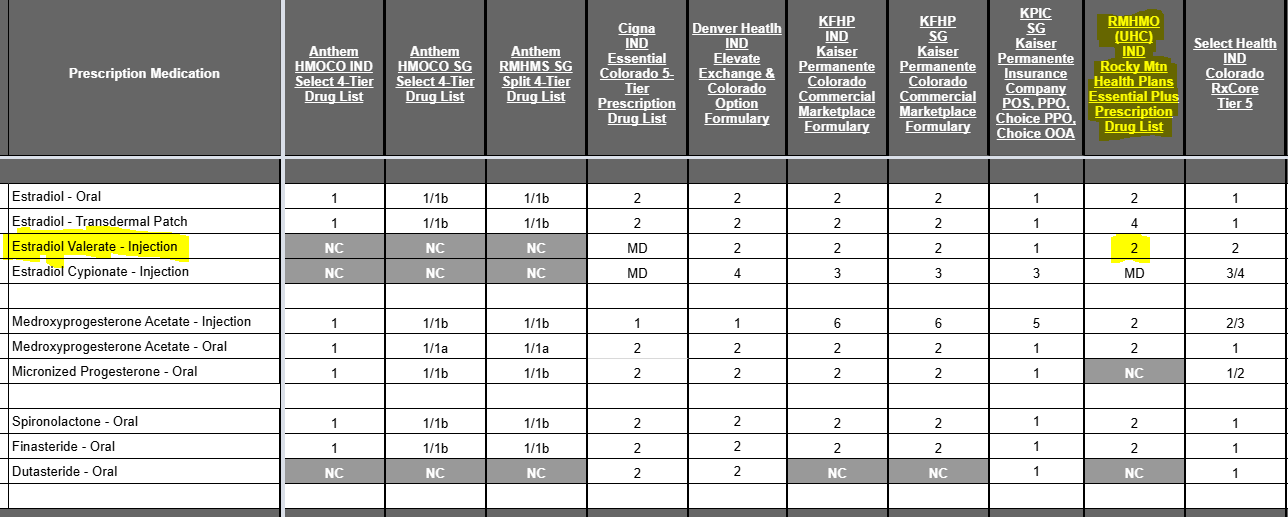
She was prescribed estradiol valerate, a standard post-operative hormone.
UnitedHealthcare rejected the prescription without valid formulary reason, telling her she didn’t “need it.”
Three separate prior authorization attempts were denied, despite the medication being listed as Tier 2 on the formulary.
That denial nearly collapsed her hormone levels. She began to spiral. She rationed what she had.
And when she could no longer take it, she called.
During that call, she invoked:
The phrase “Deny. Defend. Depose.” — not as a threat, but as a legal critique of the insurance industry’s standard playbook.
The reference to “nine more CEOs” — highlighting the depth of corruption.
The metaphorical “bang bang” — as rhetorical punctuation, not threat.
The exhausted phrase “I kinda mean that” — signaling bitterness, not intent.
This was rage born of survival, not violence born of intent.
B. The 35-Day Gap: A Timeline That Destroys Their Defense
HIPAA’s emergency exception under 45 C.F.R. § 164.512(j) requires immediacy. If UnitedHealthcare truly believed Samara was an imminent danger:
Why did they wait thirty-five (35) days before disclosing anything?
Why did they fail to initiate a wellness check, crisis outreach, or follow-up call?
Why was law enforcement contacted only after Samara began formalizing legal claims?
Here is the timeline:
November 2024: Estradiol injection denied multiple times.
Late November: Distress call placed. Metadata and speech flagged.
December 12, 2024: Samara’s OB/GYN successfully pushes through oral estradiol prescription.
No further contact from Samara. No follow-up. No police incident.
January 2025: UnitedHealthcare discloses PHI to Grand Junction Police—with no legal process and no clinical basis.
This wasn’t protection.
This was retaliation.
C. The PHI They Handed Over
To justify its contact with police, UnitedHealthcare disclosed:
Samara’s gender identity and surgical history.
Her mental health diagnoses and medication list.
Her call recordings and internal sentiment scores.
A biased internal narrative painting her as unstable and threatening—even though no clinical evaluator or crisis professional ever agreed.
This disclosure:
Violated 45 C.F.R. §§ 164.502(a), 164.512(j), and 164.514(d).
Breached Colorado’s anti-discrimination and privacy laws.
Created a permanent law enforcement record based on false inference.
D. Why They Did It: Reputation Management, Not Safety
UnitedHealthcare didn’t act to protect Samara or others. They acted to protect themselves:
They had denied a necessary medication.
They had documented the denial in internal systems.
They knew she was building a legal case.
They feared she would go public—which she later did.
By reframing her as a threat, they:
Shifted focus from their own misconduct.
Preemptively discredited her narrative by making her appear unstable.
Created a chilling effect: that any further speech might result in police attention.
They didn’t protect the public.
They protected their liability exposure—by sacrificing the liberty, dignity, and rights of a trans survivor.
E. The Stakes: From Retaliation to Precedent
If this is not challenged, it becomes a template:
For insurers to report difficult patients as threats.
For gender identity, psychiatric disability, and legal speech to be treated as red flags.
For the medical-to-carceral pipeline to operate in silence—under the false flag of “healthcare compliance.”
UnitedHealthcare tried to imprison a trans girl—not with a police raid, but with strategic metadata, selective narrative framing, and retaliatory PHI disclosure.
This is how administrative erasure becomes carceral erasure.
And unless it is exposed, it will happen again.
IV. Gender, Neurodivergence, and the Weaponization of Sarcasm
Samara Dorn was not arrested. But by all indications, she was supposed to be.
UnitedHealthcare set the machinery in motion:
They recorded and flagged her language.
They contacted multiple government agencies, including DHS and the Grand Junction Police Department.
They transmitted deeply sensitive health records to law enforcement in violation of privacy laws.
And they built an internal narrative designed to frame her as a potentially dangerous individual.
Yet somehow—miraculously—that final, devastating outcome didn’t happen.
There was a wellness check, BUT,
No knock at the door.
No arrest or citation.
By either logistical failure, lack of follow-through, or sheer grace of circumstance, the last link in the carceral chain was never completed.
But the attempt was real.
And the threat it created was lasting.
A. Misreading Identity: Trans + Neurodivergent = “Instability”
Samara is transgender.
She is neurodivergent, with a long-documented history of trauma, PTSD, ADHD, and autistic traits.
She speaks with directness, dark humor, and emotionally charged metaphor—particularly under pressure.
To a trained ear—or even a trauma-informed listener—her words would have been obvious:
A warning, not a threat.
An indictment of power, not a plan of harm.
A cry for justice, not a call to violence.
But UnitedHealthcare didn’t hear her.
They scanned her.
They flagged her.
And then they interpreted her through algorithmic, cisnormative, and ableist lenses.
Her sarcasm became evidence.
Her advocacy became instability.
Her diagnoses became justification.
The result was a profiled composite of threat—one she didn’t even know had been constructed until long after it was acted upon.
B. “Bang Bang” as Rhetorical Crime
The phrase “Bang bang” was the tipping point.
Not because it meant violence. But because it made UnitedHealthcare uncomfortable.
They did not take it as a metaphor for systemic collapse.
They took it as a threat, despite:
No mention of weapons.
No direct target.
No indication of plans, timing, or intent.
In any other context, this would be dismissed as hyperbole, gallows humor, or political critique.
But coming from a trans woman in distress—on the heels of surgical recovery, denied medication, and documented protest—it was interpreted through the worst possible lens.
This is how corporate systems weaponize tone over truth.
C. How Trans Rage Gets Labeled a Threat
Trans people—especially trans women—are expected to:
Remain calm while being denied basic care.
Stay polite while being misgendered or dehumanized.
Advocate for survival without sounding too angry, too assertive, or too defiant.
Samara didn’t follow that script.
She raised her voice.
She used legal phrases.
She connected dots others ignored.
And she named the executives whose decisions harmed her.
That was the real threat—not what she said, but who she refused to be:
A compliant patient.
A silent survivor.
A background statistic.
For that, UnitedHealthcare didn’t call a psychiatrist.
They called the police.
D. Retaliation Without Arrest Is Still Retaliation
The fact that Samara wasn’t arrested doesn’t absolve UnitedHealthcare.
It indicts them more clearly.
Because without an actual threat, the disclosure of her PHI to police had no justification.
There was no emergency.
There was no good-faith belief of imminent harm.
There was only a corporation looking to preempt liability by creating a paper trail of “compliance.”
By contacting DHS and local police without legal basis, UnitedHealthcare:
Chilled her speech.
Created a false criminal record in police databases.
Endangered her future interactions with law enforcement, medical providers, and ublic institutions.
That’s not just unethical—it’s unlawful.
And had the final link in the chain activated, she would not be telling this story today.
E. Luck Is Not a Safeguard
This case cannot be dismissed with “well, nothing happened.”
Because something did happen:
A corporate actor attempted to disappear a trans woman by reclassifying her as a security threat.
They failed not because they chose restraint, but because they didn’t finish what they started.
That isn’t a success story.
That’s a warning.
V. The HIPAA Paper Trail They Can’t Justify
How UnitedHealthcare Violated Federal Privacy Law and Left No Legal Cover
UnitedHealthcare didn’t just overreact. They broke the law.
By disclosing Samara Dorn’s protected health information (PHI) to law enforcement—without warrant, subpoena, or patient authorization—they triggered strict federal requirements under HIPAA’s emergency disclosure exception, codified at 45 C.F.R. § 164.512(j).
But what makes this more than a policy breach—what makes it legally actionable—is this:
They can’t produce any of the documentation the law requires.
Because it never existed.
A. What HIPAA Requires for Emergency Disclosures
The “imminent threat” exception to HIPAA is narrow. It is not a blanket permission slip. Under 45 C.F.R. § 164.512(j)(1)(i), a healthcare entity may only disclose PHI without consent if:
It has a good-faith belief the disclosure is necessary to prevent or lessen a serious and imminent threat to health or safety;
The disclosure is made to a person or entity reasonably able to prevent or lessen the threat;
Only the minimum necessary information is disclosed;
The basis for the disclosure is documented contemporaneously.
UnitedHealthcare’s disclosure fails all four.
B. Failure #1: No Imminent Threat
The triggering phone call occurred in late November 2024.
The PHI disclosure to Grand Junction Police occurred in January 2025—over a month later.
That’s not imminent.
There were:
No additional calls from Samara.
No threats, specific or implied.
No police incident, check-in, or behavioral escalation.
The only “event” during that time was Samara obtaining her medication legally—through oral estradiol after her OB/GYN intervened.
By the time the disclosure occurred, there was no active situation at all.
There was only a patient who had survived a manufactured crisis—and was beginning to prepare litigation.
C. Failure #2: Wrong Recipient, Wrong Role
HIPAA allows disclosures only to entities “reasonably able to prevent or lessen the threat.”
Instead of referring the matter to:
A psychiatric crisis team,
A medical safety officer,
A clinical evaluator,
UnitedHealthcare sent Samara’s PHI to the Grand Junction Police Department.
Not a clinician.
Not a court.
Not even a mandated treatment professional.
And no steps were taken to verify:
Whether the police had jurisdiction to act,
Whether Samara was under threat herself,
Whether there was any actual danger.
This was retaliation by proxy—not lawful emergency intervention.
D. Failure #3: No “Minimum Necessary” Standard
Rather than provide only the specific, targeted detail required for safety intervention, UnitedHealthcare released:
Her full gender transition history, including surgical notes;
Psychiatric diagnoses unrelated to the alleged concern;
Medication records, including controlled substances;
Call logs and transcripts, selectively excerpted to paint her as unstable.
This was a data dump, not a safety disclosure.
The “minimum necessary” standard under 45 C.F.R. § 164.514(d) was flagrantly violated. They didn’t tailor the disclosure—they weaponized it.
E. Failure #4: No Good-Faith Documentation
HIPAA requires that the disclosing entity document its belief that a disclosure is necessary and legal. This must be contemporaneous and must outline:
Why they believed a serious threat existed;
Why disclosure was the only option;
What alternatives were considered;
Who authorized the release.
Samara Dorn has reviewed all available internal records, public filings, and CORA responses. No such documentation has been produced.
Why?
Because it likely doesn’t exist.
Because this wasn’t a safety decision—it was a compliance panic response.
F. Consequences Under Federal and State Law
These failures are not harmless. They are legally significant.
Under HIPAA and HITECH:
Civil penalties may be imposed for wrongful disclosure;
“Willful neglect” without correction can trigger maximum-tier penalties;
Individuals harmed by wrongful disclosure may bring claims under state privacy and consumer protection laws.
Under Colorado law, UnitedHealthcare may also be liable for:
C.R.S. § 25-1-802(1)(a) – Unlawful release of medical records;
C.R.S. § 12-245-220(4) – Abuse of mental health privilege;
10 CCR 2505-10-8.735 – Gender-affirming care discrimination.
In total, the company did not just violate Samara’s privacy—they fabricated a justification, weaponized her health data, and risked her liberty to protect their image.
VI. A Model of Erasure: How Bureaucracy Becomes Violence
What happened to Samara Dorn was not an isolated incident. It was not a misunderstanding. It was a prototype—a chilling example of how bureaucracy becomes violence when corporate systems are allowed to:
Profile vulnerable people,
Misinterpret distress as danger,
And use metadata, not medicine, as the final judge.
UnitedHealthcare did not invent this method. But they perfected it—by disguising structural retaliation as routine compliance.
A. Administrative Erasure by Design
Samara was not “erased” by accident.
She was erased administratively.
Her prescription was denied.
Her medical history was turned against her.
Her speech was reframed as criminal.
Her identity was leveraged as a justification for surveillance.
This is administrative erasure: the systematic removal of a person’s legitimacy, autonomy, and access to services through technical, procedural, and bureaucratic means.
No bullets.
No handcuffs.
Just silence. Delay. Redirection. And escalation.
B. Policy as Weapon: The Corporate Detachment Mechanism
Every step UnitedHealthcare took had a veneer of legitimacy:
The call was flagged using “compliance risk metrics.”
The escalation was reviewed through “national security referral pathways.”
The PHI disclosure was coded under “emergency exception” tags.
But underneath the policy? Intent.
They knew Samara was preparing a legal complaint.
They knew she was a trans woman with a psychiatric record—someone the system would more easily discard.
They knew she had already called attention to Luigi Mangione, the disgraced executive referenced in her call.
They saw not a threat—but a liability.
So they acted.
They invoked DHS.
They reached out to police.
They rewrote her into something she wasn’t.
And the most haunting part?
No one had to say the word “retaliation” out loud.
The system was built to do it silently.
C. When Metadata Replaces Medicine
Samara’s call was not evaluated by a clinician.
It was analyzed by a compliance system.
Her voice was not heard—it was scored.
Her sarcasm, tone, keywords—these became algorithmic inputs.
The metadata tagged her as a threat before anyone understood her words.
This is what happens when AI-driven profiling and corporate surveillance logic replace medical judgment:
Rage becomes instability.
Protest becomes danger.
Identity becomes red flag.
The people designing these systems are not trained in trauma, neurodivergence, or gendered survival speech.
They are trained in risk minimization and legal deflection.
And so, medicine is replaced by metadata.
Care is replaced by containment.
And patients—especially trans ones—become targets, not clients.
D. The Illusion of Neutrality
One of the most dangerous features of bureaucratic erasure is that it wears a mask of neutrality.
No one at UnitedHealthcare had to raise their voice.
No one had to file false police charges.
No one had to write “we want her arrested.”
Instead, they let the system do it for them:
Escalation protocols.
Keyword flags.
Referral templates.
PHI push notifications.
This creates plausible deniability:
“We were just following protocol.”
“It wasn’t personal.”
“We had concerns for her safety.”
But protocol without clinical basis is not neutral.
It’s malicious.
It’s erasure by spreadsheet.
It’s violence by checkbox.
E. The Carceral Bureaucracy Is Already Here
What happened to Samara Dorn is not hypothetical. It is not future dystopia.
It is present reality.
Her medical distress was converted into a threat score.
Her protest was recorded, tagged, and referred to Homeland Security.
Her personal records were dumped into a local police system with no due process.
She survived by accident, not by protection.
This is the new model of carceral control—where:
Healthcare corporations act as informants,
Mental health records become tools of containment, and
Transgender speech is policed by metadata, not law.
Unless stopped, this model will spread.
VII. Conclusion:
They Tried to Imprison Me. I Survived. Now I’m Naming It.
They tried to imprison me.
Not with handcuffs.
Not with charges.
Not with a trial.
They used something quieter. Something colder.
A compliance form. A metadata tag. A law enforcement contact form.
They called me dangerous—not because I made a threat, but because I made a point.
I said: “Deny. Defend. Depose.”
That wasn’t violence. That was legal strategy.
I said: “Nine more CEOs. Bang bang.”
That wasn’t intent. That was bitter sarcasm.
I said: “I kinda mean that.”
That wasn’t instability. That was truth.
And for that, UnitedHealthcare:
Escalated me to the Department of Homeland Security,
Disclosed my PHI to the Grand Junction Police Department,
Invented a justification 35 days after the fact,
And tried to frame me as a threat to silence my claims.
They weaponized my gender.
They pathologized my voice.
They turned my medical survival into a compliance event—and my protest into a criminal suspicion.
I was not arrested.
But let’s be clear: that was luck, not mercy.
They built the pipeline.
They primed the disclosure.
They pushed the button.
Only the last switch failed to flip.
I Wasn’t Supposed to Survive With My Voice Intact
They weren’t just trying to make me disappear physically.
They were trying to discredit me before I ever spoke publicly.
To label me “unstable” so my story wouldn’t land.
To leave just enough doubt that if I went public, I’d look dangerous, not credible.
But I documented everything.
I kept the metadata.
I traced the DHS contact.
I read the HIPAA regulations.
I filed the CORA requests.
I built the timeline they thought I wouldn’t survive long enough to expose.
Now This Is Permanent
This paper is not just my story.
It is a warning to every trans person, every psychiatric survivor, every activist flagged by a call transcript or metadata score:
Your voice is not the threat.
Their systems are.
UnitedHealthcare tried to erase me with procedure.
Now I erase their plausible deniability—with truth.
I am not a criminal.
I am not unstable.
I am not silent.
I am the witness you tried to delete.
I am the patient you mislabeled.
I am the trans woman you flagged for police instead of care.
And this document—this public record—is the thing you feared most:
I named it.
I survived it.
And now the world knows.
📚 Read More
 The Story They Don’t Want Told
The Story They Don’t Want Told



 What you see above is seven unopened vials of estradiol valerate. That’s 35mL—because I don’t trust them. Because I don’t feel safe. Because if United takes this away again, the consequences wouldn’t just be clinical. They’d be existential.
What you see above is seven unopened vials of estradiol valerate. That’s 35mL—because I don’t trust them. Because I don’t feel safe. Because if United takes this away again, the consequences wouldn’t just be clinical. They’d be existential.